This Clinical Guide will help you:
– Understand the visual appearance of different nutrient quantities.
– Gain perspective of different units: micrograms (mcg), milligrams (mg), and grams (g)
– Review common clinical dosage ranges for key nutrients.
– Understand the form, timing and combinations for optimum efficacy.
Instructions:
1. You must Login to your account to access the Dosing Explorer.
2. It is best viewed at full screen using a web browser such as Chrome (PC) or Safari (Mac)
3. Use your Mouse Scroll-Wheel over the chart to zoom in and out (move away from chart to scroll the entire page).
4. Left Mouse Click, hold, and drag to move around the chart.
5. You can view where you are on the chart in the viewing window at the bottom left.
6. Click the ‘Reset‘ button at the bottom right if you get lost or would like to view the whole chart at-a-glance again.
Note 1: Use Your Judgement
Always use your own judgement (based on your own qualified education, academic research, and clinical expertise) to arrive at all dosing and prescription decisions on behalf of patients.
Note 2: Start Low
If unsure about the appropriate amount to use in a given patient and situation, always start at the lower end of the scale, and increase ONLY as symptoms and/or clinical testing demonstrates the need to. The goal is always to find the LOWEST effective dose (which will therefore also have the lowest cost and chance of interfering or adverse effects on overall optimum balance).
Note 3: Clinical Range Relevance
The ranges shown are for Clinical Use only (most begin well above general RDA levels).
The ranges begin at the lowest meaningful amount (that would be expected to provide basic clinical benefits).
The ranges then span up to the highest amounts that might conventionally be used for certain acute or intensive clinical interventions.
The ranges are a general guide only (specific situations may still call for more or less).
The ranges are intended for Adults only (see Child Dosing below).
The range values reflect the TOTAL amount taken per day (in a 24 hour period).
(Although some doses would benefit from being divided into smaller portions throughout the day to maintain body levels)
Note 4: Lower Vs Higher Ranges
Some nutrients can be used in larger quantities than others.
Some have a wide range of potential doses, whereas some are more narrow in their acceptable use.
Each often have more general uses (for achieving general sufficiency for optimum body function), as well as specific targeted therapeutic uses (doses intended to achieve a particular clinical effect, beyond simply general nutritional requirement).
For Nutrients with 2 Separate Ranges:
The LOWER range constitutes doses commonly prescribed for long term use.
(and without any confirmations from clinical lab testing)
The HIGHER range constitutes doses that may be prescribed for specific intensive interventions.
(usually temporary, and/or verified for safety and efficacy via clinical lab testing)
Note 5: Magnitude of Scale
Please note that the visual representation of the scale in this chart increases in Orders of Magnitude.
i.e.
each ‘concertina point’ (squiggle) of the scale represents an increase of 10x magnitude
(so that micrograms can be represented all the way up to grams in the one scale)
To better understand quantity units and their relative scale see the Quantity Calculator here: wmed.link/Quantities
The ‘Nutrient Dosing Explorer’
Your Guide To Better Clinical Nutrient Dosing
Access Restricted to Practitioner Members Only
Already a Practitioner Member? Login Here
If not… Signup Here
How To Dose Kids?
The General Rule for Child Nutrient Dosing
Numerous complex mathematical formulas have been developed and proposed for guiding child dosing in healthcare (such as ‘Clark’s Rule’ and ‘Young’s Rule’), however most were developed for use with pharmaceutical medications, where differences of minute quantities can be critical in the way something foreign to the body will be metabolised.
When it comes to the clinical dosing of nutrients that are more natural to the body, a more general rule is often more appropriate (and practical to remember and apply). Here is a general rule you might find useful.
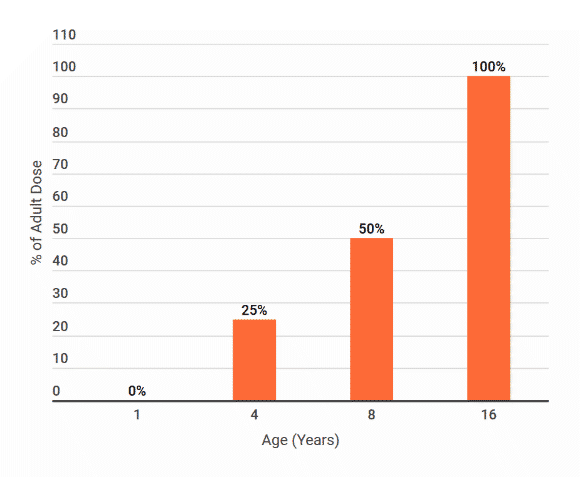
The Rule of ‘Halves for Halves’
A) First, identify what would be the appropriate starting dose for an adult. (e.g. see guide)
B) Then, for dosing purposes, consider:
16+ yrs = Full adult dose
8 yrs = Half that (1/2 adult dose)
4 yrs = Half again (1/4 adult dose)
2 yrs = Half again (1/8 adult dose)
<2 yrs = Caution *
Note:
This guideline still requires the usual clinical judgement to adjust the dose for the specific patient in question. (depending on their body weight, level of development, health, needs and known tolerance)
i.e.
Whilst 16+ may be considered metabolically adult for nutrient dosing purposes, a child that has developed faster or slower than their peers, to have a physique/function that puts them at the higher or lower end for their age, or an overweight individual with large amounts of body fat that is going to need more of any fat-soluble nutrients, or an individual with a gallbladder removed, fatty liver or general issues digesting fat, may NEED more, but can only tolerate less, and therefore dividing the doses of any fat-soluble nutrients throughout the day is going to be more necessary.
This applies when determining doses for the ‘in-between’ ages of the halves.
(i.e. do they seem closer to the previous or the next step in the dosing guide?)
* Below the age of 4 years, infants should not usually be given precise doses of highly active nutrients.
i.e.
Beyond perhaps some wholefood supplements (like fish oil, green powders, probiotics, protein and simple amino acids, …),
avoid dosing highly complex, potent or refined formulas in very young children without strong clinical justification (usually clinical need, with lab testing and monitoring).
Clinical Dosing Tips
Vitamins (Water Soluble)
TOXICITY RISK: LOW – Risk of excess from high doses is very low (most can be readily excreted via urine, beyond what the body needs)
DOSING FREQUENCY: HIGH – Usually best taken at multiple times in the day (divide daily dose to as many times as practical)
| Nutrient | Notes |
|---|---|
| Vitamin B1 (Any Form) |
Not commonly used as a therapeutic compound on its own (with the exception of the novel form ‘Benfotiamine’), however ensuring ample supply of any form, helps numerous core aspects of cellular metabolism and body function. |
| Vitamin B2 (Any Form) |
As cofactor to FAD, B2 facilitates many key cellular processes. Supplying ample ‘active’ B2 in the form ‘Riboflavin-5-Phosphate‘ (R5P) can ensure widespread metabolic and functional support for optimum health. The higher clinical dosage range is only indicated for those with certain genes, metabolic situations to overcome, and potentially migraine treatment) |
| Vitamin B3 (Niacin / Nicotinic Acid) |
Niacin is the form of B3 that causes ‘flush’, which may be distressing or uncomfortable to many (and can even occur at relatively low doses). The HIGHER clinical dose range is used almost exclusively for blood Cholesterol lowering effect (due to lipid metabolism impairment) – however in addition to the severe flush effects, this can cause liver damage over time, and has not demonstrated a substantial reduction in CVD risks (making the benefits of this intervention questionable in those without hereditary hypercholesterolemia). These aspects may lead Niacin to be the lesser desirable form of B3 to use clinically. |
| Vitamin B3 (Niacinamide / Nicotinamide) |
As an ‘activated’ form of B3, Niacinamide does not cause notable flush in most patients, and is far better tolerated at higher doses. It is not as readily associated with liver damage, even at high doses, and will fulfill every role required of B3 in the body, with the exception of not lowering liver cholesterol levels. This makes Niacinamide the ideal vitamin B3 form of choice for almost all clinical situations. Given B3’s role as a cofactor for NAD, cellular health and function relies heavily on ample supply of B3. B3 has therefore been indicated for anti-aging, energy production and other broad benefits to the body. In particular, the HIGHER clinical dosage range has been used in various novel clinical applications such as anxiety & mental health, inhibiting skin cancer progression, and balancing immune system dysregulation (reduces infection as well as autoimmune progression such as Arthritis). Note B3 is also used for ‘mopping up’ excess methyl molecules in those prone to overactive methylation (or when supplementing high dose methyl nutrients). It is best to start small (such as 100mg – splitting a capsule if necessary) in those with fragile methylation metabolism, and then working up to the effective dose (often between 250-500mg) in those that might benefit from the added methyl regulation or who are receiving intensive methylation support treatment. |
| Vitamin B5 (Any Form) |
The ‘Pan’ in ‘Pantothenic Acid‘ means ‘everywhere’ (due to it being widespread in nature), making this molecule very familiar to the body, and widely needed for daily metabolism (especially steroid hormone metabolism). It also makes it very well tolerated, with no common ill effects reported, even when taken in very large amounts for very long periods of time. Some clinical situations that justify the HIGHER clinical dosage ranges include: support for general Steroid Hormone metabolism, Cortisol production (Adrenal support), and most notably, reliably ameliorating skin Acne. |
| Vitamin B6 (Pyridoxine) |
The simple Pyridoxine form of B6 must be converted to P5P in the body in order to be substantially metabolically active. This slightly cheaper form of B6 is associated with a risk of Peripheral Neuropathy (permanent nerve damage) from very high doses for extended periods of time (months). It is therefore potentially a less desirable form of B6 to use clinically. |
| Vitamin B6 (P5P) |
Pyridoxal-5-Phosphate (P5P) is the ‘activated’ form of B6 found in the body, and when taken supplementally, even in large doses, has not been demonstrated to cause Peripheral Neuropathy in the way that Pyridoxine has. P5P fulfills all the roles of B6 in the body (which are many and diverse), and is therefore considered the preferable form of B6 to use clinically. The HIGHER dosage range may be indicated for those with pronounced needs for nervous system support, overcoming elevated Pyrroles, along with many other metabolic and hormonal support functions. |
| Vitamin B9 (Folinic Acid) |
Folinic Acid is a more natural and ‘activated’ form of Folate than synthetic Folic Acid, and limits the risk of excess methyl molecules, by still requiring conversion to 5MTHF as and when required by the body to fulfill all metabolic needs for Folate. This makes Folinic Acid the ideal default choice of Folate to use clinically in all individuals who have not been clinically tested to justify using the pre-methylated form 5MTHF which has certain limitations associated with it. Note: Since supplemental Folinic Acid usually constitutes a racemic mixture, it is only half active. This means that any target doses of folate may require double the amount of Folinic acid to be achieved. |
| Vitamin B9 (5MTHF) |
As the fully ‘activated’ form of Folate, 5MTHF provides potent activity in the body, however also delivers exogenous methyl groups to the body (overriding the body’s ability to regulate how much 5MTHF is produced), it may therefore be more prone to adverse reactions or even inhibition of the Folate Pathway if taken in higher doses or for long periods or in those with compromised metabolic pathways) – making this form desirable ONLY in situations that call for it, and perhaps for pulsed temporary periods, on the basis of metabolic testing to verify the need, along with monitoring progress (it may therefore be preferable to use Folinic Acid in all other situations that Folate is clinically indicated) |
| Vitamin B12 (Any Form) |
As the core form of B12 in the body, Hydroxycobalamin fulfills all the roles of B12 in the body and can be converted to Adenosylcobalamin for energy production etc., or methylated (by activated Folate) to form Methylcobalamin which facilitates methylation throughout the body. For this reason Hydroxycobalmin may be the most versatile and well tolerated form of B12 to use clinically in all situations that do not specifically call for one of the other forms to focus in their one area of metabolic activity. Higher doses of B12 are generally well tolerated, even in large amounts for long periods (as is indicated in cases of long standing dietary or digestive deficiency), however some may experience an exacerbation of Acne symptoms (which may require higher dose B5, or a reduction in the B12 dose, to resolve) Note: Since B12 functions in close relationship with Folate, it may often be advisable to supply an equal dose of B12 with all Folate doses (and vice versa), until biochemical testing can demonstrate which is needed in greater amounts (altering the ratio accordingly). |
| Vitamin C (Ascorbic Acid) |
Since humans do not posses the enzyme to synthesise Ascorbic Acid (like many other animals do), it’s regular and frequent supply to the body’s metabolism may provide many functional benefits. However saturation of absorption and metabolism mechanisms may occur at relatively moderate doses, making it desirable, if not important, to get small frequent doses throughout the day (rather than large doses in one sitting) for optimum effects. Doses between 100mg-500mg divided throughout the day, provide almost all general benefits of Vitamin C supply. However, certain clinical situations do justify the higher dosage ranges (such as for Cardiovascular protection, Adrenal Support, etc…) |
Vitamins (Fat Soluble)
TOXICITY RISK: MODERATE – Potential risk of excess when taken in very high doses for long periods, without confirming need/status.
DOSING FREQUENCY: LOW – Always best taken with any meal containing fat (however daily dose can usually be taken in one sitting)
| Nutrient | Notes |
|---|---|
| Vitamin A (Retinoids) |
With the RDA for adults approaching 700-1,000 mcg, and it being assumed that at least some will be coming from various forms in the diet, 300 mcg (1,000 IU) of Retinol may be considered the starting point of supplementation, and due to the narrow therapeutic window, 3,000 mcg (10,000 IU) is then considered the upper limit (beyond which risks of teratogenesis may occur if consumed during the first trimesters of pregnancy). For these reasons it is rarely indicated to supplement Retinol in doses over 3,000 mcg (unless medical condition, along with proven absence of pregnancy, and liver function tests demonstrate a safe basis to proceed). Note: Any high doses of Vitamin A should always be accompanied by a proportionate amount of supportive Vitamin D (to ensure optimum balanced function as well as minimise the risk of toxicity). |
| Vitamin A (Carotenoids) |
Since the biological conversion of Beta-Carotene (the most converted of all Carotenoids to Vitamin A (Retionoids)) is at best 10:1 but in some instances may be as poor as 28:1, the need for dietary Carotenoids may be substantially higher than Vitamin A itself, in order to achieve healthy Vitamin A levels in the body. For these reasons Carotenoid supplementation may be ineffective in certain individuals (even at high doses), and may present a risk when taken from synthetic supplements (e.g. lung cancer demonstrated in some limited trials) – for this reason it is perhaps advisable to always obtain small amounts of natural Retinoids (e.g. Cod Liver Oil) as the best choice of Vitamin A supplementation, rather than synthetic Beta-Carotenes. Note: Amounts over 30,000 mcg per day can accumulate to cause Carotenoderma (orange skin) from unconverted/unutilised Carotenes. This will subside after ceasing intake and may have no adverse affect when obtained from food (however excess refined forms may ironically interfere with Vitamin A metabolism) |
| Vitamin D (D3) |
Cholecalciferol (Vitamin D3) is technically a steroid hormone rather than a typical dietary vitamin (10-250 mcg = 400-10,000 IU). It therefore has some of the most numerous and varied activities in the body (with almost every cell possessing a receptor for it), some of which affect genetic programming. This makes sufficiency of this nutrient incredibly important, and a high clinical priority to ensure in almost all conditions. One of Vitamin D’s key roles is facilitating Calcium absorption, and therefore higher doses of Vitamin D may result in higher blood Calcium levels. To prevent inappropriate deposition of this Calcium (e.g. calcification of the arteries in CVD) it is advisable to always combine any high doses of Vitamin D with Vitamin K (which assists with optimum Calcium distribution and metabolism in the body) e.g. 100mcg of Vitamin K for every 125mcg (5,000 IU) of Vitamin D. Note: Vitamin D and Vitamin A have a mutually supportive but also competitive relationship in many mechanisms of the body (the Vitamin D receptor works in tandem with Vitamin A). It is therefore often important to include some amount of Vitamin A with all high doses of Vitamin D, and vice versa. |
| Vitamin E (Tocopherols) |
As a key fat-soluble stabiliser of cell membranes, ‘Vitamin E’ is often referred to as Alpha-Tocopherol. But it is in fact comprised of 8 isoforms (4 Tocopherols and 4 Tocotrienols – Alpha-Tocopherol being only one of these). Furthermore there are synthetic forms of Alpha-Tocopherol (DL-Alpha-Tocopherol) that have very different levels of activity (and metabolic consequences) to the natural form (D-Alpha-Tocopherol) which has a conversion of 1mg = 1.49 IU (or 0.67mg = 1 IU). For these reasons when seeking a Tocopherol based Vitamin E supplement, it may be wise to seek only natural (D) forms and one that includes a mix of the other forms (especially Gamma-Tocopherol, not solely Alpha) when fat-soluble antioxidant support is indicated clinically (as in anti-ageing, CVD, etc.). |
| Vitamin E (Tocotrienols) |
Tocotrienols are a largely overlooked family of the Vitamin E forms, due to often being found in much smaller amounts, than most Tocopherols, in foods. However more recent research suggests that they may actually have more unique and profound activity at smaller quantities than the Tocopherols and therefore represent a useful form to consider for clinical interventions (beyond simply meeting sufficient dietary Vitamin E levels). Note: There is no ‘IU’ equivalency for Tocotrienols, and they may compete with Tocopherols for uptake and activity in the body (for this reason they should be supplemented away from Tocpherols – and lower amounts may be used for greater effect). |
| Vitamin K (K2) |
Vitamin K is key in almost all forms of Calcium metabolism (from bone mineralisation to blood clotting). Whilst there are multiple forms of Vitamin K, K2 is often considered the most ‘natural’ or ‘active’ in the body. K2 can be further divided into various isoforms, with MK7 being perhaps the most active in certain tissues such as bone, and MK4 being better utilised by most other soft tissues (therefore possibly preventing calcification in tissues such as arteries). It may therefore be prudent to use MK7 as the fundamental form for meeting basic Vitamin K needs, with the first 100mcg being the most effective. Although amounts greater than that have also been shown to be very safe (there has been no notable toxicity level established for Vitamin K), however the added benefits of going above 200mcg may be minor. |
Minerals (Elemental)
TOXITY RISK: VARIED – Some more than others (however balance more than level may be key)
DOSING FREQUENCY: MODERATE-HIGH – Minerals should be dosed as water-soluble nutrients in order to meet ongoing metabolic needs.
| Mineral | Notes |
|---|---|
| Calcium (Ca) |
Calcium has a widespread need throughout the body (not just for structural integrity, but also as a cofactor in muscle and nervous system function, etc.). Due to these high needs for Calcium, unlike many minerals, the body has a large reservoir of stored Calcium (i.e. Bones) that ensure ongoing supply. It is important that when not in transit or being utilised, Calcium is not deposited in soft tissues (otherwise there can be an increased risk of kidney stones, spurs, and the arterial sclerosis of CVD). Vitamin K is essential for optimising this Calcium distribution and metabolism and would therefore be a helpful addition to any high Calcium intake/supplementation. However Calcium’s functions often also rely on a balance with Magnesium. Therefore co-prescription with at least equal amounts of Magnesium whenever supplementing Calcium may also be key. Calcium and Magnesium Citrates are both highly effective sources of these electrolyte macro minerals. |
| Magnesium (Mg) |
Magnesium has one of the most universal roles in hundreds of metabolic pathways in the body. However unlike Calcium, Magnesium does not have such a vast reservoir to maintain ongoing metabolic supply with (although bones do also contain, and require, some Magnesium). Additionally, certain situations such as periods of high physical or psychological stress may increase losses/demands of Magnesium. For these reasons it may be as clinically important to obtain as much, if not more, Magnesium than Calcium in any supplementary regime. Magnesium Citrate provides the most efficient method of taking Magnesium. However Magnesium Orotate may have unique benefits for the cardiovascular system, and Magnesium Threonate stands alone as potentially the superior form for supporting nervous system function (by delivering Mg to the CNS via the BBB better than almost all other forms). |
| Zinc (Zn) |
The biochemical demand for Zinc in the body is not only as prevalent as it is Magnesium, the two minerals often work together in the same pathways, supporting each other. Therefore deficiencies of both Magnesium and Zinc are common. However the ‘Zinc Tally’ taste test is an unreliable method for determining sufficiency, and RBC blood tests should be used to confirm status in the absence of any overt deficiency signs to indicate it sooner. Like with Magnesium, Zinc Citrate is a highly efficient form to take, however Zinc Picolinate may be retained and utilised particularly well by those with compromised digestion, metabolism or nervous system function (themselves all common reasons to take Zinc). |
| Copper (Cu) |
Copper is the key counterpart mineral to Zinc, with Zinc deficiency and Copper excess being the most common imbalance to present clinically, making Copper supplementation rare. Although there may be 10-20% of certain populations who will present with the opposite, and justify Copper supplementation – or are deficient in both and warrant some Copper in addition to Zinc (often a 10:1 ratio of Zn:Cu). Therefore since Copper excess is common (and highly oxidative/damaging to tissues), it is imperative to thoroughly test Copper status (via blood Copper & Ceruloplasmin (Copper Binding Protein) levels) BEFORE supplementing any Copper, as well as after any prolonged high-dose Zinc supplementation. Niacin chelated Copper may be the ideal form to use whenever a need for Copper supplementation has been demonstrated. |
| Iron (Fe) |
Like Copper, Iron is highly oxidative and damaging to tissues when in excess. However unlike Copper (which is often execssive) it is far more common to be deficient in Iron and actually need supplementation support. However it remains best practice to ALWAYS test blood Iron, Transferrin & Ferritin (Iron Binding Protein) levels, BEFORE supplementing any form of Iron. Note: prescription forms of oral Iron often contain Ferrous Sulphate which is not an ideal form of iron (as it is not absorbed well during digestion and therefore can cause severe constipation) it can be more effective and comfortable for the patient (also with less potential for oxidation damage in the body) to use amino acid chelated forms of Iron such as Ferrous Bisglycinate. It is rarely wise to go over 50mg of elemental Iron per day, and always best to divide such high doses into multiple serves throughout the day. |
| Iodine (I) |
Iodine has crucial functions within the body, and yet deficiency remains common in developed nations. This often most notably effects Thyroid function, however also has implications for other body tissues such as the brain and breast tissue, where it balances estrogen hormonal function. For this reason almost everyone can benefit from some amount of Iodine supplementation (at least a few hundred mcg) to ensure adequate levels. However due to the highly oxidative nature of Iodine, and its complex distribution and storage mechanisms within specific tissues of the body, it may be most prudent to not dose more than 1,0000 mcg per day without performing urine Iodine testing, and perhaps blood Thyroid hormone testing, to confirm needs and status before increasing further. In certain situations however it may be readily demonstrated that mulitple mg doses are necessary and beneficial to individual patients. Potassium Iodide is acceptable as a stable form of Iodine for supplementation, however free Iodine itself may be distributed differently or to different tissues, making a liquid mixture of both Iodides and Iodine potentially the optimum form to dose Iodine (this has been made available, albeit in very potent doses, within ‘Lugol’s Solution‘ at compounding pharmacies for some time). |
| Manganese (Mn) |
Being a trace mineral cofactor needed in only small amounts (with potential for excess in some cases), Manganese is not commonly dosed individually. However it provides a key role in various important pathways of the body (such as the core antioxidant enzyme SOD, bone integrity, glucose tolerance / Insulin function, and prevention of seizures). For these reasons its inclusion in any multi mineral or trace mineral supplement is highly beneficial for many, to ensure general nutritional sufficiency of this important mineral. Although some acute high dosing may also be justified for physiological effect in certain clinical situations involving the above mechanisms. (competition with Iron and Magnesium may need to be taken into account and levels monitored in such cases) |
| Molybdenum (Mo) |
Molybdenum is another often overlooked but highly important trace mineral that plays a key cofactor role in numerous key enzymes throughout the body such as ‘Sulfite oxidase‘ (sulfite preservative tolerance), ‘Xanthine oxidase‘ (viral immune function, antioxidant defense and Uric Acid metabolism), ‘Aldehyde oxidase‘ (CYP450 and MAO neutransmitter metaoblism), and ‘Mitochondrial amidoxime reducing component’ (cellular detoxification and energy production). Ensuring general sufficiency of this important trace mineral through quality multi mineral and trace mineral supplements would be beneficial for most individuals. Certain genetic polymorphisms that impede any of the above enzymes may justify higher specific dosing of Molybdenum, in order to optimise biochemical metabolism. (Note: High doses of Molybdenum for long periods of time may suppress Copper levels in the body and induce deficiency. This may be a beneficial temporary use of Magnesium (along with Zinc) in cases of excess Copper – monitor levels accordingly). |
| Chromium (Cr) |
The trace mineral Chromium has a primary metabolic role as a cofactor in the correct functioning of Insulin receptors. For this reason ensuring general sufficiency of Chromium (through very small mcg amounts per day) may help ensure optimum Insulin function for some individuals. However many with already impaired glucose tolerance or Insulin Resistance (Diabetes II) may need higher doses in order to compensate for their compromised Insulin function, and to restore healthier blood glucose levels (this may help with weight management, food cravings, energy levels, cardiovascular risk, etc.), and a high glycemic diet and lifestyle may more rapidly deplete existing Chromium levels, justifying higher doses to maintain effects. It is however possible to get too much Chromium, making Chromium Nicotinate one of the most preferred forms to use clinically (as it has a potentially more favorable metabolic profile and has demonstrated less adverse effects than Chromium Picolinate in this regard). |
| Selenium (Se) |
Selenium is a trace mineral with one of the most important functions within the body, yet is needed in one of the smallest amounts of all nutritional trace minerals. Selenium serves as a cofactor (often working in tandem with sulphur bearing compounds such as Methionine and Cysteine) to the synthesis and metabolism of the body’s primary antioxidant, detoxification and anti-aging enzyme: Glutathione, as well as other important and widespread body metabolites such as Thyroid hormone. This makes any deficiency of Selenium potentially very impactful to the overall health of the body, and clinical restoration of even basic levels (e.g. 50 mcg a day) potentially powerful, within the broader support of numerous health conditions. With one of the narrowest therapeutic windows of all supplemental nutrients, an excess of selenium can also be damaging to the body, leading the Australian Therapeutic Goods Administration to specify warnings on all doses over 150 mcg a day (in contrast to the American regulatory system readily supporting 200-400mcg per day) due to some acknowledgement of the likely amounts also being contributed by the diet. Given it’s Suplur affinity, Selenomethionine provides one of the most stable and well metabolised forms of supplemental Selenium to choose (with better retention and metabolism properties than non organic forms such as Sodium Selenite) |